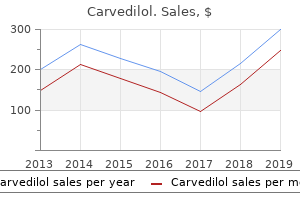
"Order carvedilol 25 mg amex, blood pressure pills make you tired".
By: Z. Masil, M.A., M.D., M.P.H.
Vice Chair, Alabama College of Osteopathic Medicine
It is set up in the Action settings to hyperlink to the slide in your presentation labelled "conclusions" blood pressure chart vaughns carvedilol 6.25 mg lowest price. When you are presenting pulse pressure 65 cheap carvedilol 12.5mg with amex, all your slides will have this small action button and when you move your mouse pointer over the button hypertension over the counter medication generic 6.25 mg carvedilol mastercard, and press the right button, the system will automatically jump to your "conclusions" slide, no matter how many other slides are in between. And finally You should have a check list to go through before you give your presentation which will ensure that everything is in place (see Box 5. Observe what others do in their presentations and then ask how they managed to do it. It must be obvious that PowerPoint is unique in providing a phenomenally wide range of possibilities to produce a complete disaster of a presentation. However, it is a powerful communication tool which offers, at present, the ultimate to dazzle, astonish, and to hold the attention of your audience. If you cannot hold their attention, then your presentation will not make the points you wish to your audience. A further advantage is that the slides in a PowerPoint presentation are always the correct way round. In short, you’ve done about as much with it as you can, and as talks go, it is not at all bad. We’ve all had to endure speakers who can’t be heard, or who look all wrong, or who display some thoroughly irritating mannerism that completely distracts from what they’re trying to get across. Or, perhaps more realistically, how can you at least make sure that you don’t get too much in the way of your own presentation? Here are a few basic tips – most of which I have to confess I learnt the hard way – to help you avoid the likeliest own-goals. Get there early The first piece of advice is: make sure you arrive in plenty of time. The chairman looks anxiously at the clock, wondering whether to bring the coffee break forward. Stumbles onto stage, knocks over microphone, scrabbles for projector switch, shoves on first overhead upside-down, and generally kyboshes the entire proceedings. There are several advantages: • It gives you an opportunity to pick up the "mood" of the meeting and the issues that may have a bearing on your talk. Grappling with an unfamiliar sound system is a classic elephant trap for hapless speakers. The usual disasters are failing to switch on the microphone, failing to make sure that it’s pointing in the right direction, constantly clunking the lead, or speaking so closely that you sound like a Dalek with laryngitis in a thunderstorm. Spend a few minutes before your session starts to do a sound check – and if necessary make a few adjustments. If you’re using a microphone on a stand– either a floor-stand, table-stand or fixed to the podium – adjust it so that it’s pointing at your mouth, but is positioned slightly to one side of the direct line of fire of your breath as you speak. This is to avoid "popping" – those periodic explosions accompanying every "P" that punctuates a presentation. The microphone should be about 6 in (15 cm) from your mouth, and on the side nearer the screen because if you happen to turn your head away from it, to look at the screen for example, your voice may disappear. Instead of the time-worn "testing, one, two, three, testing", I would recommend "Peter Piper picked a peck of pickled pepper" to sort out the pops from the snaps and crackles. The lapel microphone may be a marvel of miniaturisation, but it can cause tons of trouble. First, there’s the agony of where to clip it – a particular challenge for presenters without lapels. Women often find themselves in this awkward situation – and occasionally have to resort to holding the thing in position. With a radio microphone, the box of works can provide an even more difficult problem.
Doctors who have taken their specialist training in academic units often continue in university hospitals either as senior lecturers with honorary consultant status or as NHS consultants prehypertension uptodate purchase discount carvedilol, some become NHS consultants in district general hospitals heart attack normal blood pressure buy 6.25 mg carvedilol with amex, and a few go into clinical research or management in the pharmaceutical industry hypertension over the counter medication cheap carvedilol 6.25 mg. The NHS does not have different levels of seniority of consultant but it does reward exceptional service and scientific distinction with distinction awards, salary supplements which at the highest level are substantial in relation to the basic salary. Not all doctors in the hospital service aspire to become consultants; they may become an associate specialist, part time medical officer (clinical assistant), hospital practitioner, or staff doctor, a grade established for those who have not completed a formal specialist training programme or do not wish to have the full range of responsibilities of a consultant. These posts are advertised nationally in the same way as all other medical posts in the NHS, with the exception of preregistration house officer posts linked with particular medical schools which are filled internally. If their earnings from private practice exceed more than 10% of their NHS salary, they must give up part of their NHS salary. Their status as a specialist in private practice is underwritten by the fact that they have obtained a consultant post in open competition after a full period of rigorous training. A curious and peculiarly English myth has long promoted the public belief that solely private practitioners in Harley Street are the best. The reverse is likely to be true because most practitioners who do not also work as consultants in the NHS have not completed an accredited specialist training or, if they have, have not obtained a consultant post in open competition, with the exception of a few who have already been NHS consultants and have given up their public service to work solely in private practice. There is nothing to stop any doctor fully registered with the GMC from setting up as a private specialist, but in future doctors not listed on the specialist register will not be eligible for payment as a specialist through insurance schemes. They may also find it difficult to satisfy Royal College’s expectations that they are regularly keeping up to date in their relatively isolated position. Appraisal and revalidation Whatever the specialty, all registered medical practitioners will in future be regularly appraised in the context of their work to ensure that they are maintaining satisfactory standards. This has become the norm in other professions and there is no reason for doctors to be an exception, except that it has been difficult to devise an appropriate and efficient way of undertaking appraisal in clinical specialties without creating a whole new work agenda for very busy people. Every five years, the portfolio of a doctor’s appraisals will be submitted as evidence for revalidation of registration with the GMC. Again, there is a formidable need to devise a system which is practical, cost effective, and sufficient to maintain confidence in the profession. Many have no firm intentions at this stage beyond knowing a few areas which they have discounted. For most this gives them time to settle on their intended career options and keep a healthy perspective on their life, and it is no longer regarded unfavourably by many employers. Career opportunities Medicine offers an amazing range of different career options. Medical students are well advised to take a careful look at the very broad canvas of opportunity before they qualify. Most people finally choose their specialty within two or three years of graduation. However an increasing number of doctors choose careers which are more varied,include other interests, and are flexible enough to allow them to fit their career around their life,not the other way round. This includes at least 12 months as a GP registrar; two periods of at least six months each in educationally approved training posts drawn from a list of hospital specialties particularly relevant to general practice, such as paediatrics, care of the elderly, obstetrics and gynaecology, psychiatry, and accident and emergency; and the remainder of the time in hospital or community medicine. Any or all of the training may be undertaken part time provided the whole process is completed within seven years. Training is carefully and continuously supervised by specially trained and accredited general practitioners, who guide and monitor training through a process of summative assessment.
Generic 12.5 mg carvedilol fast delivery. high blood pressure ki dawa| high blood pressure treatment| high blood pressure ka ilaj।tabletgyan.
How many times have I heard Blaine say that he didn’t know what he would do if I had a poor attitude about Parkinson’s hypertension over 60 carvedilol 25 mg visa. Of course pulse pressure medscape cheap carvedilol 12.5mg otc, we all have bad spells blood pressure medication make you tired 12.5mg carvedilol with visa, but learning how to deal with them is the most important thing. For example, after I have done a certain amount of housework and feel wound down and achy all over, I know it is time to sit down and relax with a maga- zine or a cup of decaffeinated coffee. When I’m depressed, I try to spend an hour visiting someone whose company I enjoy. I’ve noticed that even patients who are confined to wheel- chairs can have positive attitudes. An eighty-six-year-old lady came to our support group meetings faithfully for five years, and the last two of those years she was in a wheelchair. She always said such nice things about her daughter and other caregivers, and they always said such nice things about her. Mark Flapan, a psychologist in New York City, has writ- ten with great insight about the role that attitude plays in Parkin- son’s disease. His article, "Living with Parkinson’s: What You Can Do for Yourself," in the Autumn 1989 issue of the PDF Newsletter, speaks to each one of us: Your Mental Outlook Makes a Difference Even if you or your doctor can’t do any more for your disease than you are doing, you can still do more for your life. You can always learn to live better with Parkinson’s since how you live with your illness comes from your mental outlook—and your mental outlook is something you can do something about. What’s most important in your mental outlook is how you view and judge yourself as a person with Parkinson’s. As it hap- pens, how you view and judge yourself can undermine your life as much as your illness can—maybe even more. Possibly you believe you got Parkinson’s because you didn’t take proper care of yourself over the years, or you did something harmful to your body. If that’s attitude makes all the difference 59 the case, you know something the doctors don’t know, since medical research has yet to find the cause of Parkinson’s. Maybe you believe Parkinson’s is God’s punishment for bad behavior—although you don’t know what you did that was bad enough for you to deserve this. I realize that religions have taught that disease is punish- ment for sinful behavior. If you’re troubled by this thought, I suggest you talk to a pastoral counselor of your religion or read Rabbi Kushner’s book When Bad Things Happen to Good People. You undermine your life if you feel guilty because you think you are a burden on your family. Even though Parkinson’s has affected your family, it isn’t as though you’re deliberately doing something by being sick. When it comes to an illness, there is a big difference between doing something and being something. Furthermore, it’s only by chance that Parkinson’s is in your body rather than in the body of some other family member. After all, it could have been your marital partner who got the disease instead of you. But no matter which member in a family happens to get a chronic illness, the whole family is affected, and each family member has to cope with the illness in some way. Just as you didn’t do anything to get Parkinson’s, you can’t do anything to make it go away. Therefore, you’re not responsi- ble for the physical effects of your illness on your family. But you are responsible for the effects of your mental outlook on your family, because this is something you can change. You undermine your life if you de- value yourself as a person because you have Parkinson’s—if you view Parkinson’s as a weakness, a stigma, something to be ashamed of, rather than as a biological happening.
Thus hypertension synonym carvedilol 12.5 mg sale, its creation and presentation held numerous levels of meaning blood pressure up heart rate down purchase generic carvedilol line, both personal and col- lective heart attack quizlet order carvedilol. It was therefore important to process and discuss the image on a deeper level than the creator’s statement ("Jimmy makes beautiful things, and in case we have to add this to another project I want him to do it"). This symbolic process even- tually ended with the artist saying, "All my life I’ve lived like this. As with other directives in this chapter, Yalom’s (1983) sentence completion tasks provide an excellent foundation upon which art therapy projects can be based. In this case, the group was struggling with significant life issues surrounding a sense of competency offset by the comfort and lethargy of dependency. Thus, I gave the group directives focused on per- sonal change in the hope that these topics would motivate the clients not only to interact but to take action against the fears that threatened to over- whelm their fragile sense of self. One personal change directive I offered the group was to draw "the dif- ferences between your personality now and your personality five years ago" (Yalom, 1983, p. However, it was the drawings completed by two ac- tively recovering alcoholics (Figures 6. This drawing illustrates the complexity of emotions concern- ing his drinking—from the confidence gained (and now lost) in social sit- uations to the distress associated with blackouts and multiple arrests. The client had recently begun to discuss and accept the problems associated with his heavy drinking. These two art tasks produced the greater part of feedback as the group members actively processed the vicissitudes of change, motivation, and daily living. In these discussions personal growth was identified by the group members as a desired goal but one out of reach as fear and apathy again overtook the group consciousness. In response to these pervasive emotional struggles I adapted another di- rective from Yalom (1983) and instructed the group to draw "a change you would like to make but don’t think you can. This figure was completed by a young adult who suf- fered from auditory hallucinations secondary to a traumatic head injury. Due to profound cognitive disturbances, his impaired executive func- tioning capabilities (planning and organizing) and significant memory impairments often impeded his participation in group sessions. He would frequently require numerous sheets of paper, forget the directive, or perse- verate on a single detail. In the discussion that followed, group members shared issues related to their lifelong struggle to attain symptom relief. For some, medication pro- vided liberation from their delusional and often disorganized symptoms; for others, medication negated that which made them special and unique (see Figure 6. Ultimately, for this group member the artwork paved the way to a shared feelings expression that would have been nearly impossible to initiate ver- bally. Additionally, it allowed his peers to empathize with, appreciate, and accept another’s perspective through a supportive interpersonal experi- ence. Self-Disclosure In the last structured exercise we will review, self-disclosure is the foun- dation upon which interpersonal interactions between group members 265 The Practice of Art Therapy rest. Yalom (1985) specifies that "the self-disclosure may involve past or current events in one’s life, fantasy or dream material, hopes or aspirations for the future, and current feelings toward other individuals" (p. As with any art therapy interaction, the active leader stance produces total group communication, from the individual creation to the process- illuminating questions; focus on a group-centered model is always fore- most. For this individual and collective group investment promotes a sense of community, understanding, and intimacy, which we hope will be gener- alized into the larger environment. This depressed adult had a propensity to render his draw- ings in black, devoid of adequate detailing. Additionally, he only found success or glory through his delusional religious beliefs. Thus, his mood- incongruent psychotic features and his symbolic renderings afforded him a 6.