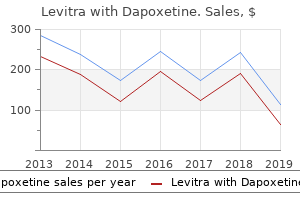
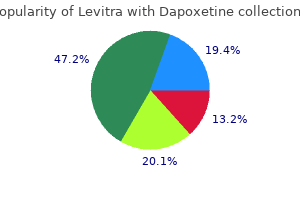
"Discount levitra with dapoxetine 40/60mg online, erectile dysfunction hypertension medications".
By: F. Keldron, M.B. B.CH. B.A.O., M.B.B.Ch., Ph.D.
Clinical Director, Louisiana State University School of Medicine in New Orleans
The etiology of this condition is diverse erectile dysfunction 43 years old discount levitra with dapoxetine 20/60mg visa, and may occur in association with fractures of the hindfoot erectile dysfunction 32 years old 20/60mg levitra with dapoxetine with visa, rheumatoid arthritis erectile dysfunction treatment doctors in hyderabad levitra with dapoxetine 40/60mg otc, 93 Peroneal spastic flatfoot – tarsal coalition or bony fusion of the bones of the hindfoot (tarsal coalition). Without question, the vast majority of cases seen are associated with tarsal coalitions. It is likely that the condition occurs in less than one percent of the population, and is nearly always seen at the time of adolescence and puberty. The most common coalition is that between the calcaneus and the navicular (Figure 5. Oblique radiograph clearly demonstrating calcaneal navicular Clinically the condition presents as a painful bar (tarsal coalition). The presence of a painful stiff foot in the adolescent age range should immediately alert the physician to the possibility of a tarsal coalition. The diagnosis is then established by appropriate radiographic examination of the Figure 5. Computed tomography image demonstrating medial facet talocalcaneal coalition. If clinical suspicion is not satisfied, then a CT scan of the hindfoot is indicated, and is probably the most accurate means of determining the presence or absence of a hindfoot coalition. Although conservative treatment in the form of casting and orthotics is occasionally successful, the vast majority of patients will become recalcitrant, and continue with symptomatology, warranting surgical intervention. Current surgical management includes the use of operative procedures designed to separate the coalition by resection of the bar, or fusion of the joints involved (triple or subtalar arthrodesis). Surgical treatment has been successful in roughly 90 percent of all cases. The primary physician’s role is to be cognizant of the clinical presentation and to institute appropriate orthopedic referral. Adolescence and puberty 94 Recurrent subluxation (dislocation) of the patella Recurrent subluxation, or dislocation of the patella, is a condition most commonly seen in adolescents and teenagers, most commonly occurs in females, with a definite familial background. A congenital form is recognized and is most commonly associated with other disorders or syndromes (Down syndrome, skeletal dysplasias, Ehlers–Danlos syndrome, and arthrogryposis). When seen in its most common form it is nearly always associated with generalized ligamentous laxity. In association with ligamentous laxity there is evidence of contracture of the lateral soft tissue supports of the patella, particularly the lateral retinaculum and capsule and vastus lateralis Figure 5. Abnormal patellar “tracking” seen during knee extension in tendon insertion. The most common presenting symptoms are that of episodes of “giving way” with pain in the knee and occasional “popping. The source of these symptoms is believed to be due to the malalignment of the patella within the femoral intercondylar groove, and most likely is related to a roughened area on the patella “rubbing” onto the synovial surface. The diagnosis is established by examining the “tracking” of the patella as the knee is brought from full flexion into full extension. Commonly a “figure four” sign is seen, or a “Q” sign, which relates to the movement of the patella within the intercondylar groove as the knee is brought into full extension (Figure 5. In full extension it is usually 95 Pain syndromes of adolescence possible to displace the patella laterally with very little pressure (light thumb pressure). Provocative pressure on the patella in an attempt to sublux the patella laterally will often elicit “guarding” or apprehension on the patient’s behalf. Not uncommonly, there will be tenderness over the medial capsule and retinaculum on direct pressure. Although radiographs may be occasionally helpful in discerning the relative degree of formation of the lateral condyle and the position of the patella within the groove, the diagnosis is established on a clinical basis. Long-term disability encountered with this condition relates to the degree of subluxation and dislocations and the length of time the dislocations have been occurring.
Communication of pain is accomplished via verbal and nonverbal channels (e impotent rage definition cheap levitra with dapoxetine 40/60 mg otc. This chapter discusses research on the ex- pression of pain erectile dysfunction questionnaire uk order levitra with dapoxetine from india, including the importance of the entire communicative rep- ertoire and the potential for deception erectile dysfunction rap lyrics levitra with dapoxetine 20/60mg fast delivery, the judgmental skills and biases of potential allies and antagonists, and the advantages and disadvantages of current social systems designed to care for people communicating painful distress. Issues related to the communication of pain within families are covered, as are matters pertaining to populations with limited ability to communicate (e. Following the first part of the book that is largely focused on theoretical work, Gibson and Chambers outline important developmental consider- ations in the psychology of pain. Pain expression and experience transform with aging, reflecting ontogenetic maturation, socialization in specific famil- ial and cultural settings, and the impact of experiences with pain. An under- standing of the cognitive, affective, behavioral, and social challenges con- fronted during the various stages of life from birth to terminal illness is required. The earliest and latest stages of life presently carry substantial INTRODUCTION 9 risk of unnecessary or undermanaged pain because of an inadequate knowledge base, underdeveloped assessment procedures, and inadequate pain management. This chapter examines and systematizes developmental processes in pain experience, expression, and communication. A major source of individual differences (other than biological matura- tion) is culture. The chapter by Rollman considers the empirical and theo- retical literature on the impact of culture on the experience and expression of pain, delineating observed differences and ethnocultural variations in the meaning of pain. There is a focus on mechanisms responsible for varia- tions (acculturation and socialization), linking them to the biopsychosocial model. Individual differences in response to comparable tissue stress and injury are systematically related to known factors (gender, health anxiety, other personality traits). The chapter by Skevington and Mason provides a re- view of the literature and a model of social factors impacting on pain in an effort to understand the origins of individual differences. The role of intrapersonal factors such as self-efficacy and their relationship to outcomes and recovery from pain are also considered. The next section of the book addresses clinical issues more directly than the preceding chapters. The role of psychological assessment among pre- and postsurgical pain pa- tients is discussed. Bruehl and Chung move the book into an intervention focus with a state- of-the-art discussion of psychologically based interventions for acute pain (wounds, burn, other soft tissue injuries, fractures, medical procedure pain, etc. Psychological interventions represent a neces- sary feature of multidisciplinary care for patients suffering from chronic pain and pain-related disability. This chapter examines the most commonly employed approaches to the treatment of chronic pain as well as the empir- ical evidence (or lack thereof) pertaining to their efficacy. Widely used cog- nitive/behavioral approaches are featured, but psychodynamic perspec- tives are also examined. The manner in which medication usage relates to 10 HADJISTAVROPOULOS AND CRAIG psychological treatment (e. More- over, a discussion of how psychological interventions can be applied with postsurgical and presurgical pain patients is included. The last section of the volume focuses on current controversies and ethi- cal issues. Craig and Thomas Hadjistavropoulos reviews current controversies, including critical analyses of the definition of pain, frequent unavailability of psychological interventions for chronic pain, the use of self-report as a gold standard in pain assessment, fears about the implementation of certain biomedical interventions and others.
One should suit the RPE to the are specific and occur only in the overloaded muscle individual on a specific mode of exercise and not groups or muscles (Durstine and Davis erectile dysfunction yoga youtube buy generic levitra with dapoxetine 20/60mg online, 2001) how to get erectile dysfunction pills purchase levitra with dapoxetine 40/60mg free shipping. It should be used only as a guideline in set- for Resistance Training: ting the exercise intensity (Franklin et al erectile dysfunction doctor dallas trusted 40/60mg levitra with dapoxetine, 2000b; A 5–10-min warm-up period consisting of aerobic Pollock et al, 1998). The goal is to develop total for that individual and achieves the desired outcome body strength and endurance in a time-efficient manner given the time constraints of the exercise session. Mode: The prescription should include a minimum The ACSM recommends 20–60 min of continuous of 8 to 10 separate exercises that target major muscle aerobic activity. Free weights and weight machines are multiple, short-duration exercise sessions <10 min commonly used; however, springs, surgical or rubber with frequent interspersed rest periods. Intensity/Duration: Perform a minimum of one set musculoskeletal and cardiovascular risk with exer- of 8 to 12 repetition of each of the exercises to the cise performed at high intensities for short dura- point of volitional fatigue. Volitional fatigue refers tions as compared with lower intensity exercise to the inability to move a resistance through the for a longer duration (Franklin et al, 2000b; Pollock appropriate range of motion with proper mechani- et al, 1998). A set of 10 to 15 repetitions is recom- mended for developing muscular endurance and Frequency for those who are older or frailer (Franklin et al, The ACSM recommends that aerobic exercise be per- 2000b). Frequency: Perform these exercises 2 to 3 days per Less conditioned people may benefit from lower week, usually with a day of rest in between intensity, shorter duration exercise performed at (Franklin et al, 2000b). Additional Recommendations status, individual goals, and compliance rate. Perform every exercise through a full range of Frequency, intensity, and/or duration can be increased motion using proper technique and in a con- to provide overload. Maintain a normal breathing pattern and avoid breath holding (Valsalva). Exercise with a partner when possible to pro- Overload and specificity are precepts of resistance train- vide feedback, assistance, and motivation ing. Overload occurs when a greater than normal phys- (Bryant and Peterson, 2001). Muscular strength and endurance are developed by MUSCULOSKELETAL FLEXIBILITY TRAINING increasing the resistance to movement or the frequency or duration of activity to levels above those normally Stretching Techniques experienced. A training intensity of approximately Static stretching: Static stretching involves slowly 40–60% of one repetition maximum appears to be stretching a muscle to the point of mild discomfort CHAPTER 13 BASIC PRINCIPLES OF EXERCISE TRAINING AND CONDITIONING 81 and then holding that position for an extended period 3. Cool-down (5–10 min): This phase provides a period of time (usually 10 to 30 s). It is effective, requires of gradual recovery from the endurance phase and little time and the risk of injury is low. This type of stretch can While endurance training activities should be per- result in muscle soreness or injury and is generally not formed 3 to 5 days a week, complementary flexibility recommended (Franklin et al, 2000b; Fredette, 2001). Flexibility prioceptive neuromuscular facilitation (PNF) involves training can be included as part of the warm-up or a combination of alternating contraction and relax- cool-down, or undertaken at a separate time. It is effective, but it is days when endurance training is not; however, both time consuming, requires a partner and may cause activities can be combined into the same workout residual muscle soreness and has potential for injury (Franklin et al, 2000b; Wygand, 2001). RATE OF PROGRESSION The recommended rate of progression in an exercise- ACSM Recommendations for Flexibility Training conditioning program depends on functional capacity, Flexibility exercises should be performed in a slow, medical and health status, age, individual activity pref- controlled manner with a gradual progression to erences and goals, and an individual’s tolerance to the greater ranges of motion. For apparently healthy adults, active warm-up precede vigorous stretching exercises the endurance aspect of the exercise prescription has (Franklin et al, 2000b; Fredette, 2001). Mode: A general stretching routine that exercises maintenance (Franklin et al, 2000b; Wygand, 2001). Intensity: Stretch the muscle to a position of mild The initial stage should include light muscular discomfort.
We consider the abduction method because of the need to keep a child in a pants to be inadequate as a maturation treatment after plaster cast in such a barbaric position for months dislocation what causes erectile dysfunction in diabetes purchase levitra with dapoxetine 40/60 mg. We do (Albert Lorenz writing about the bloodless reduc- not usually administer a maturation treatment exclusively tion and immobilization method developed by his during the night erectile dysfunction doctor in jacksonville fl order levitra with dapoxetine in india. The treatment is only Fettweis : In 1968 Fettweis proposed a treatment suitable if the parents are cooperative and intelligent impotence after 40 order levitra with dapoxetine canada. Various statistical analyses have Complications after conservative treatment shown that the rate of avascular necrosis is much lower, Avascular necrosis of the Femoral head at around 5%, with the squatting position than with The commonest and most serious complication of treat- the Lorenz position at approx. The long-term ment of congenital dislocation of the hip is avascular treatment with the Fettweis cast is also very well toler- necrosis of the femoral head. Age is not a relevant factor for this in untreated hip dislocation, it is very rare in this context. In most cases, the necrosis is a consequence of treatment Another major advantage of cast treatment is the op- and does not result from the dislocation itself. The ne- timal compliance, which avoids the risk of the child being crosis can occur in the epiphyseal plate either laterally, moved out of the ideal position for prolonged periods. This results in shortening of the cast for at least 8 weeks for immobilization purposes. The same shortening of the changed under light sedation and does not usually require femoral neck and overgrowth of the greater trochanter is general anesthesia. The feet do not need to be included also seen with central necrosis, whereas medial necrosis in the cast but can be allowed to move freely. But the necrosis can also affect the need not necessarily be prepared from white plaster and acetabulum. Absence of ossification of the femoral head center for more than 1 year after the reduction. Absence of growth of an existing femoral head center for at least 1 year after the reduction. Widening of the femoral neck during the year follow- 3 ing the reduction. Increased bone structure of the femoral head center on the x-ray, possibly with subsequent fragmentation. Presence of a deformity of the femoral head and neck after the end of the recovery phase (coxa magna, coxa plana, coxa vara, short femoral neck). A classification for the severity of the necrosis, presented in ⊡ Table 3. The necrosis rate depends partly on the type of re- duction and partly on the immobilization method. X-ray of a 4-year old girl after congenital hip disloca- As regards the type of reduction, the overhead method tion and lateral femoral head necrosis with lateral epiphyseal closure, appears to be associated with the lowest rate of necrosis, head-in-neck position and shortening and valgus displacement of the while the Hoffmann-Daimler brace caused the most cir- femoral neck a b c d ⊡ Fig. As regards the immobilization on the Secondary deterioration other hand, the Fettweis squatting position was by far the For a long time, doctors assumed that once a hip had most favorable method with just 2% of necroses. Necrosis returned to normal after treatment it could no longer de- rates of 16% and 27%, respectively, were recorded for the teriorate. The Pavlik harness was also recent years we have observed several cases in which a nor- associated with a fairly low necrosis rate, at 7%. Naturally, mal hip during childhood has deteriorated into a distinctly the necrosis rate after surgical treatment cannot be com- dysplastic hip during puberty (⊡ Fig.
EDX studies may alert the possibility of an Electrodiagnostic testing is not a perfect test and unsuspected concomitant pathologic process should not be performed in every athlete with neuro- (i erectile dysfunction ayurvedic drugs in india buy levitra with dapoxetine with mastercard. Nerve injury localization often needs to be logic deficits following a traumatic posterior knee dis- objectively confirmed prior to contemplating location impotence yahoo buy generic levitra with dapoxetine 40/60mg on line, which should be treated emergently) erectile dysfunction labs 20/60 mg levitra with dapoxetine fast delivery. An athlete presenting with plantar foot numb- should be kept in mind (Table 19-4). EDX studies can be used to determine if the sci- determine the degree of nerve injury. Determine the extent and chronicity of nerve nous fistula, open wound, coagulopathy, lym- injuries. SPECIFIC CONDITIONS Athletes may commonly present with tibial and per- oneal nerve problems which can be evaluated by EDX Many pain complaints in athletes present as neuro- techniques. TIBIAL NERVE Although most long distance runners do not complain of symptoms of neuropathy, they do appear to have sub- There are specific EDX techniques to evaluate the clinical changes in quantitative sensory thresholds and tibial nerve and its terminal branches (Park and Del nerve conduction velocities (Dyck et al, 1987). TABLE 19-5 Focal Entrapment Neuropathies Seen in Runners SYNDROME/NERVE SYMPTOMS ENTRAPMENT SITE Tarsal tunnel syndrome (tibial nerve Plantar pain/paresthesias, worse at night and with Under flexor retinaculum proper) prolonged standing or walking Medial calcaneal neuritis Medial heel pain At medial heel Inferior calcaneal nerve (first branch Chronic heel pain, no numbness, weakness of Between AH and QP or calcaneal heel spur of lateral plantar nerve) ADM Medial plantar nerve (jogger’s foot) Medial arch pain At master knot of Henry (hypertrophy of AH) Morton’s toe (interdigital nerve) N/T in toes At intermetatarsal ligament Superficial peroneal nerve Lateral ankle pain At deep crural fascia as exits lateral Fascial herniation compartment Deep peroneal nerve Dorsum of foot pain At inferior extensor retinaculum Tightly laced shoes Common peroneal nerve N/T in lateral leg, dorsum of foot Compression in fibular tunnel by fibrous edge of peroneus longus Traction from ankle sprains ABBREVIATIONS: N/T = numbness/tingling; AH = abductor hallucis; QP = quadratus plantae; ADM = abductor digiti minimi CHAPTER 19 ELECTRODIAGNOSTIC TESTING 117 The medial plantar nerve is easily tested as a motor Prognosis is critical if obtainable nerve conduction study, stimulating at the tibial nerve Comparison with previous EDX data whenever possible proximal to the medial malleolus and recording over the abductor hallucis. PERONEAL NERVE REFERENCES The peroneal nerve’s motor and sensory components Bachner EJ, Friedman MJ: Injuries to the leg, in Nicholas JA, can be consistently studied with nerve conduction Hershman EB (eds. Baltimore, MD, Williams & ankle, the fibular head, and the popliteal fossa. Mayo Clin Proc The sensory nerve study is performed by stimulating 62:568, 1987. Fisher MA: AAEM Minimonograph: Part 13: H reflexes and F 2 EMG REPORT waves: Physiology and clinical indications. F-wave The electrophysiologic report should include a number studies: Clinical utility (see comments). Muscle Nerve 21: of important pieces of data for the referring physician. A diagnosis of resonance imaging of the lumbar spine in people without back S1 radiculopathy by H reflex changes alone will carry pain. Leach RE, Purnell MB, Saito A: Peroneal nerve entrapment in One abnormal finding does not make the diagnosis if runners. New York, NY, Demos primary care physicians have moved away from this Vermande, 1997, p 191. But numerous evidence-based guidelines Vancouver, British Columbia, Johnson Printing Company, 1999. San Antonio, as established by the American College of Cardio- TX, University of Texas Health Science Center-San Antonio, logy (ACC) as well as the American College of 1996. Sports Medicine (ACSM) have shown that many of Wilbourn AJ, Shields RW: Generalized polyneuropathies and other the new technologies do not necessarily have better nonsurgical preripheral nervous system disorders, in Omer GE, diagnostic characteristics than the standard exercise Spinner M, Beek ALV (eds. EXERCISE TEST TERMINOLOGY INTRODUCTION It is essential to understand the basic EST terminol- Various anatomic, electric, and physiologic tests are ogy prior to performing the test (Fig. The exercise stress PR segment: The isoelectric line from which the ST test (EST) endures as one of the few valuable and segment and the J point are measured at rest. CHAPTER 20 EXERCISE TESTING 119 exercise, the PR segment slopes downward and short- content. In the absence of pulmonary disease, arte- ens in duration at which point the PQ junction rial oxygen content, and saturation generally becomes the point of reference for the ST segment. Venous oxygen content is determined by the segment depression is measured.
Cheap levitra with dapoxetine american express. Health Men - Foods to Help Erectile Dysfunction ED Treatment How to Get Harder Erections.